The Ankle Brachial Index is a standard and common method of physiologic assessment of vascular pathology in the lower limbs in a fast and simple manner.
Systolic pressures are measured in each of the right and left brachials, as well as at the level of the right and left ankles. Ankle Brachial Index, or ABI, is determined as the ratio between the higher brachial systolic pressure and each of the ankle pressures. Thus, a separate ABI value is obtained for the Right side and the Left sides.


Unlike ultrasound imaging modalities which provide anatomical information, ABI assessment provides a direct indication of the physiological severity of the vascular pathology. ABI testing machines are often used for fast and simple screening of the lower limbs, prior to determining if ultrasound imaging is required.
Measuring the Systolic blood pressure with an ABI machine is simple. Once a pressure cuff is wrapped around the measured site, a distal Doppler or Photoplethysmograph (PPG) waveform is obtained. The cuff is then inflated until the distal signal disappears as a result of the total occlusion. The pressure cuff is then deflated in a controlled manner, and the pressure at which the distal signal re-appears is determined as the systolic pressure.
Using Doppler to measure the distal waveform is the traditional and clinically accepted method, although PPG sensors are also used in specific conditions or locations.
The Falcon is considered to be the best ankle brachial index machine as it allows very simple and fast diagnosis of ABI. Simply place 4 color-coded pressure cuffs on each of the right/left brachial and ankle sites, select the ABI protocol, and you are ready to go. The ABI test can be completed in just a couple of minutes.
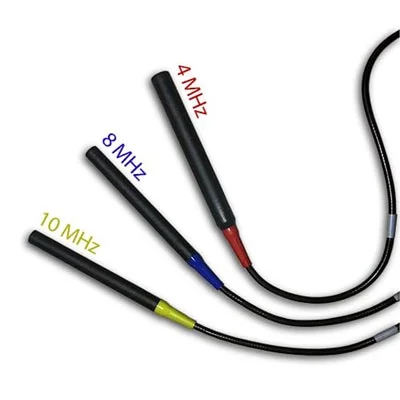
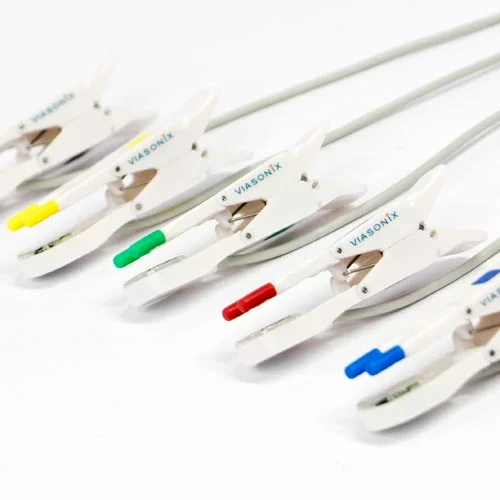
The Falcon is also known as a peripheral vascular diagnosis system as it allows you to select from a wide variety of Doppler probes and PPG sensors for best outcome. All Doppler probes, PPG sensors and pressure tubes are color coded to allow optimal user interface and correlation with the dedicated software. The target inflation pressure, as well as the deflate rate and various other parameters can be customized by the user for optimal measurements.
Numerous other features and options of the Falcon system, such as automatic cuff inflation once a signal is identified, or simultaneous measurements, display of contralateral results, and many more options, are designed to simplify the use of the Falcon ABI physiologic system in a fast and efficient way.
Once the distal Doppler or PPG waveform reappears during the deflation phase of the pressure cuff, the measurement can be stopped, and the Falcon places a cursor to mark a potential systolic pressure. The user may move the cursor to a different location, and the systolic pressure is changed accordingly. Right and left ABI are calculated automatically by the Falcon and presented clearly on the screen and in the report layout.
Gold Standard ABI Measurement Method
Secondary Method of ABI Assessment

High quality available in a variety of sizes
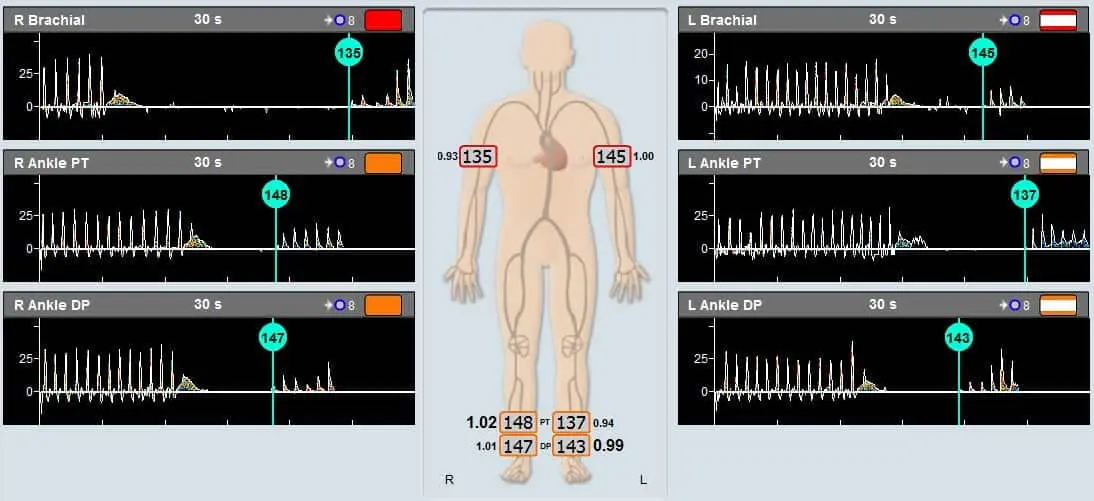
Example of an ABI test performed on a patient using Viasonix Falcon/PRO ABI Doppler machine. The sensor used in this case is an 8 MHz Doppler probe.
According to many international guidelines, such as the AHA, ABI is diagnosed and evaluated as follows:
| Range | Common Diagnosis |
|---|---|
| ABI ≥ 1.4 | Non compressible arteries |
| 1 ≤ ABI < 1.4 | Normal |
| 0.9 ≤ ABI < 1 | Borderline |
| ABI ≤ 0.9 | Abnormal |
An ABI ratio of around 1 is considered normal, while lower values indicate various levels of significant peripheral arterial disease (PAD) and higher ABI values represent incompressible arteries which are typically associated with higher vascular stiffness.
Overview of Peripheral Arterial Disease of the Lower Extremity, Ali F. AbuRahma and John E. Campbell, Noninvasive Vascular Diagnosis, A.F. AbuRahma (ed.), Springer International Publishing AG 2017, Ch 21, pp 291-318
2016 AHA/ACC Guideline on the Management of Patients With Lower Extremity Peripheral Artery Disease; A Report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines; Journal of the American College of Cardiology, Vol. 69, No. 11, 2017
Peripheral vascular disease assessment in the lower limb: a review of current and emerging non‑invasive diagnostic methods, Shabani Varaki et al, BioMed Eng OnLine (2018) 17:61
2017 ESC Guidelines on the Diagnosis and Treatment of Peripheral Arterial Diseases, in collaboration with the European Society for Vascular Surgery (ESVS), Victor Aboyans et al., European Heart Journal (2017) 00, 1–60
The Ability of the Toe-Brachial Index to Predict the Outcome of Treadmill Exercise Testing in Patients with a Normal Resting Ankle-Brachial Index, Christian Høyer et al, Annals of Vascular Surgery, Volume 64, April 2020, Pages 263-269
Association of cardiovascular autonomic dysfunction with peripheral arterial stiffness in patients with type 1 diabetes, Lía Nattero-Chávez et al, The Journal of Clinical Endocrinology & Metabolism
Measurement and Interpretation of the Ankle-Brachial Index, Victor Aboyans et al, Circulation. 2012;126:2890–2909
The effect of percutaneous transluminal angioplasty of superficial femoral artery on pulse wave features, Mikko Peltokangas et al, Computers in Biology and Medicine 96 (2018) 274–282
The Toe Brachial Index (TBI) is defined as the ratio between the systolic blood pressure in the right or left toe and the higher of the systolic pressure in the right or left arms.
TBI is a common vascular physiologic assessment test, which is taken in order to determine the existence and/or severity of peripheral arterial disease (PAD) in the lower extremities. TBI is frequently a complementary measurement to the ABI (Ankle Brachial Index) test, or it is performed when the ABI cannot be measured or if it is unreliable. TBI measurements are fast, simple, non-invasive, and painless.
The TBI measurements in the right/left toes are often taken if the ABI measurements are high (for example, above 1.3) or if the ankle’s arteries are determined as incompressible when measuring the ABI. While the ABI measurement can become unreliable when arterial stiffness increases, the TBI is less susceptible to vascular stiffness. This distinction is because an important characteristic of the digit or toe arteries is that they usually do not calcify, and therefore do not have increased vascular stiffness. Thus, the TBI is a valuable diagnostic tool when the blood vessels are stiff or incompressible, as may be the case, for example, when diagnosing diabetic patients.

Measuring the TBI is fast and simple. A toe/digit pressure cuff is wrapped around the measured toe, and a sensor, normally a Photoplethysmograph (PPG) sensor, is placed on the toe distally to the pressure cuff. In some special cases also a Doppler measurement can be made instead of the PPG measurement.
The toe pressure cuff is then inflated until the distal PPG signal flattens, indicating total arterial occlusion.
The pressure cuff is then deflated in a controlled manner, and the pressure at which the phasic PPG waveform reappears is determined as the systolic pressure.
The Falcon is designed to allow completing the TBI diagnosis in a fast and straightforward manner. All that is required is:
The Falcon provides a variety of PPG sensors that can be used to meet particular needs:
The Falcon allows performing pressure measurements in up to 5 separate toes simultaneously. For example, this will enable us to complete the right and left toe pressure measurement bilaterally to save examination time.
In the special cases where Doppler is selected for the TBI test, the Falcon allows selection from a range of Doppler probe frequencies, including the 10MHz probe for superficial penetration. All PPG sensors, probes, and pressure tubes are color-coded to allow optimal user interface and correlation with the dedicated software. The user can easily change the target inflation pressure, as well as the deflate rate and various other parameters for optimal measurements.
The TBI index appears in the examination report. If multiple toes are measured in each foot, then the separate pressure index of each measured toe is clearly displayed on the screen and included in the report.
The Falcon supports many other options and features which are designed to simplify the use of the Falcon TBI physiologic diagnostic system in a fast and efficient way. One such feature is displaying the “average” PPG waveform, which is a function of total blood flow, rather than showing only the phasic waveform. This additional curve provides a valuable supplementary criterion when determining the systolic pressure, particularly in a noisy environment.
Once the distal PPG (or Doppler) waveform reappears during the pressure cuff deflation phase, the measurement can be stopped, and the Falcon places a cursor to mark a potential systolic pressure. The user may move the cursor to a different location, and the systolic pressure is changed accordingly. R/L TBI values are calculated automatically by the Falcon system and presented clearly on the screen and in the report layout.
Secondary Method of ABI Assessment
High quality available in a variety of sizes
Although the pathologic TBI criteria are still somewhat ambiguous, a common TBI normal values range, such as presented in this study, is shown in the table below.
| Range | Common Diagnosis |
|---|---|
| TBI ≥ 0.7 | Normal |
| TBI < 0.7 | Abnormal |
Specifically, TBI < 0.7 is associated with claudication, and a TBI < 0.2 is associated with pain at rest.
The absolute systolic toe pressure is also an important diagnostic parameter. A normal toe pressure is about 30 mmHg less than the ankle pressure. A systolic toe pressure of less than 30 to 50 mmHg suggests chronic limb ischemia, according to the recommendations of the TASC group. A TBI value less than 0.5 suggests proximal arterial disease of moderate severity, while an index less than 0.2 and toe pressures less than 30 mm Hg are consistent with critical ischemia and poor potential for healing.
Overview of Peripheral Arterial Disease of the Lower Extremity, Ali F. AbuRahma and John E. Campbell, Noninvasive Vascular Diagnosis, A.F. AbuRahma (ed.), Springer International Publishing AG 2017, Ch 21, pp 291-318
2016 AHA/ACC Guideline on the Management of Patients With Lower Extremity Peripheral Artery Disease; A Report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines; Journal of the American College of Cardiology, Vol. 69, No. 11, 2017
Peripheral vascular disease assessment in the lower limb: a review of current and emerging non‑invasive diagnostic methods, Shabani Varaki et al, BioMed Eng OnLine (2018) 17:61
2017 ESC Guidelines on the Diagnosis and Treatment of Peripheral Arterial Diseases, in collaboration with the European Society for Vascular Surgery (ESVS), Victor Aboyans et al., European Heart Journal (2017) 00, 1–60
The Ability of the Toe-Brachial Index to Predict the Outcome of Treadmill Exercise Testing in Patients with a Normal Resting Ankle-Brachial Index, Christian Høyer et al, Annals of Vascular Surgery, Volume 64, April 2020, Pages 263-269
Association of cardiovascular autonomic dysfunction with peripheral arterial stiffness in patients with type 1 diabetes, Lía Nattero-Chávez et al, The Journal of Clinical Endocrinology & Metabolism
The toe-brachial index in the diagnosis of peripheralarterial disease, Christian Høyer et al, Journal of Vascular Surgery, Volume 58, Issue 1, P231-238, July 01, 2013
Inter Society Consensus Report for the Management of PAD, TASC II report (Trans-Atlantic Inter-Society Consensus), Ed. Lars Norgren and William R Hiatt, The Society for Vascular Surgery, doi:10.1016.
Peripheral vascular disease assessment in the lower limb: a review of current and emerging non‑invasive diagnostic methods; Shabani Varaki et al, BioMed Eng OnLine (2018) 17:61
Physiological examinations repeated after induced stress, typically following a specific exercise protocol, are used to differentiate between vascular disorders and determine the functional severity of stenosis. This test is particularly recommended with a borderline ABI.
An asymptomatic arterial lesion in the lower limbs may become symptomatic after induced stress.
The purpose of the exercise testing is to increase the blood flow in the legs, which in turn may result in a more considerable pressure drop distal to an arterial lesion or obstruction to flow. In this situation, the ABI (Ankle Brachial Index) will decrease post-stress testing compared to the ABI value at rest.

The induced stress protocol is usually standard and well-defined, with 5 minutes of walking on a treadmill at a pace of 2 mph (3 km/h) and at an inclination grade of 10-12 degrees, or until the patient experiences pain. Alternatively, tiptoeing or similar exercise activity may be used to induce stress.
All exercise activities must be under the supervision of the examiner. Special caution should be taken prior to deciding to perform exercise tests. There are several contraindication risk factors that should prevent a patient from performing this test, including:
Most frequently, the stress testing will include measurements of ABI or Segmental Blood Pressures, but Pulse Volume Recording (PVR) and CW Doppler measurements are also common. Segmental pressures are often measured at different post-stress times to determine the recovery time from the stress effects. Particular interest is in identifying significant variants from the resting pressure indices and, specifically, changes in the ABI.
The Falcon supports stress testing following exercise with a variety of measurements, including blood pressure measurements and ABI, Doppler, PVR, and PPG measurements. A protocol list clearly details all of the sites that were measured under rest conditions prior to exercise and marks the corresponding pressures in a graphical manner for clarity.
Furthermore, the Falcon allows an unlimited number of measurement cycles after the induced stress in order to quantify the time to recovery in a controlled manner.
The Falcon also has an easy option of adding Stress Testing “on the fly” to any examination protocol with a single button, even if this test was not previously configured or planned. This feature allows optimal clinical diagnosis when Peripheral Arterial Disease (PAD) is suspected.
The details and documentation of the induced stress are well defined. A selection is available to define the type of induced stress, such as Exercise, Cold Immersion (particularly for Raynaud’s testing), or Reactive Hyperemia (in exceptional cases when the patient is unable to exercise). All details of the exercise test are also documented, including the type of exercise and speed and inclination of the treadmill. In addition, a large digital timer displays the progress of the induced stress, the onset of symptoms during the exercise can be easily inserted, and the total duration of stress is also documented.
The Rest control measurement can be displayed on the screen while performing the Post-Stress measurement for comparison and clear clinical assessment. In addition, charts and graphical bars display the pre- and post-stress pressures for each measured site, including the corresponding pressure differences.
User configured alerts can define threshold conditions that highlight the sites with clinically significant pressure drops for optimal clinical diagnosis.
Gold Standard ABI Measurement Method

Secondary Method of ABI Assessment
High quality available in a variety of sizes
It is expected that with a significant arterial lesion, the distal pressures and the corresponding ABI value will decrease after exercise. Severe PAD is considered when the post-exercise ankle pressure drops by more than 20 mmHg. Likewise, a decrease in the value of ABI by more than 0.2 also indicates PAD.
The recovery time of the ankle pressures to baseline values after exercise is usually within 2 minutes.
Longer periods of recovery time indicate different levels of disease, such as single or multi-segment disease or resting pain, when recovery time is longer than 15 minutes.
Overview of Peripheral Arterial Disease of the Lower Extremity, Ali F. AbuRahma and John E. Campbell, Noninvasive Vascular Diagnosis, A.F. AbuRahma (ed.), Springer International Publishing AG 2017, Ch 21, pp 291-318
2016 AHA/ACC Guideline on the Management of Patients With Lower Extremity Peripheral Artery Disease; A Report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines; Journal of the American College of Cardiology, Vol. 69, No. 11, 2017
2017 ESC Guidelines on the Diagnosis and Treatment of Peripheral Arterial Diseases, in collaboration with the European Society for Vascular Surgery (ESVS), Victor Aboyans et al., European Heart Journal (2017) 00, 1–60
Noninvasive Physiologic Vascular Studies: A Guide to Diagnosing Peripheral Arterial Disease, Robert C. Sibley et al., RG • Volume 37 Number 1, pp 352-355
Peripheral vascular disease assessment in the lower limb: a review of current and emerging non‑invasive diagnostic methods; Shabani Varaki et al, BioMed Eng OnLine (2018) 17:61
Nonimaging Physiologic Tests for Assessment of Lower Extremity Arterial Disease, Marsha M. Neumyer, in “Introduction to Vascular Ultrasonography”, Ed. Pellerito and Polak, Elsevier Health Sciences, 2012, Ch 14, pp 244-261
Disclaimer of Information & Content
The content of Viasonix Ltd. website is for information only, not advice or guarantee of outcome. Information is gathered and shared from reputable sources; however, Viasonix Ltd. Management is not responsible for errors or omissions in reporting or explanation. No individuals, including those under our active care, should use the information, resources or tools contained within this self-diagnosis or self-treat any health-related condition. Viasonix Ltd. Management gives no assurance or warranty regarding the accuracy, timeliness or applicability or the content.
In special cases, the reactive hyperemia test (RH) can replace the standard exercise tests and induce vascular stress.
The Reactive Hyperemia test is allowed only in certain countries.
Stress testing is frequently used in peripheral vascular diagnosis to differentiate between different vascular disorders, or to determine the functional severity of an arterial stenosis. Systolic pressures are measured before and after inducing vascular stress. While typically the patient is asked to perform a physical exercise such as exercise on a treadmill, sometimes the patients have difficulties in performing exercise.
RH requires the inflation of a pressure cuff in order to occlude the blood flow to the limb or segment of interest for up to several minutes, and then rapidly releasing the cuff pressure in order to generate the hyperemic effect.
It is crucial that a professional examiner will be present near the patient at all time, and immediately deflate the pressure cuffs when necessary.